

Upper-Incisor Position as a Determinant of the Ideal Soft-Tissue Profile
Michael A Webb, Frank E Cordray, P Emile Rossouw

Introduction
Facial esthetics remains a cornerstone of contemporary orthodontics. The upper incisor, often viewed as a functional and structural anchor, also plays a pivotal role in determining facial harmony. In this 2016 study by Webb, Cordray, and Rossouw, the authors explore how the upper incisor's position relates to soft-tissue planes defined by the forehead and glabella, offering practical insights into orthodontic treatment planning for improved esthetics.
Background and Study Objective
Traditional cephalometric analyses prioritize bony and soft-tissue landmarks for evaluating facial esthetics. However, these methods often overlook the upper incisor as a central reference point. This study investigates whether planes defined by the soft-tissue forehead and glabella can reliably position the upper incisor to achieve an ideal soft-tissue profile.
Key Question: Can the upper incisor's anteroposterior (AP) position serve as a determinant of facial harmony?
Materials and Methods
Patient Selection
Sample:
Initial pool: 400 Caucasian adolescents post-fixed appliance therapy.
Final selection: 64 patients (33 females, 31 males) with Class I occlusions, balanced profiles, and normal overjet/overbite.
Criteria for inclusion: At least three of four ABO-certified orthodontists rated their profiles as esthetically pleasing.
Data Collection
Cephalograms and Photographs:
Digital lateral cephalograms captured in natural head position (NHP).
Standardized photographs (profile, frontal, and smiling).
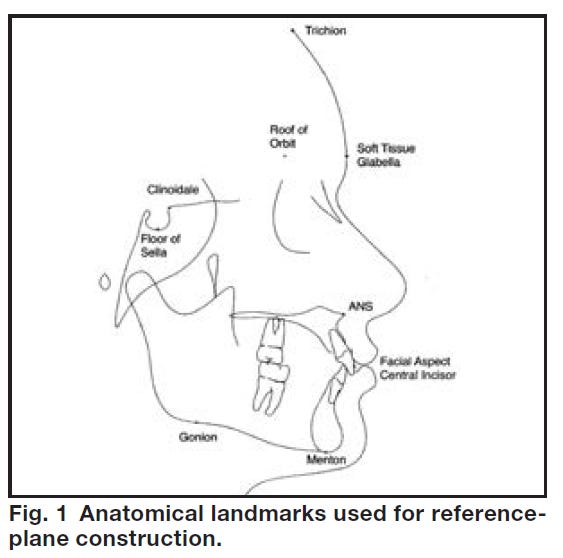
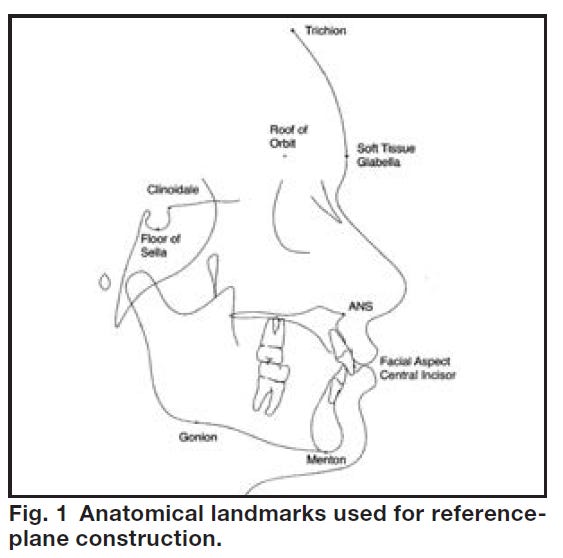
Landmark and Plane Definitions:
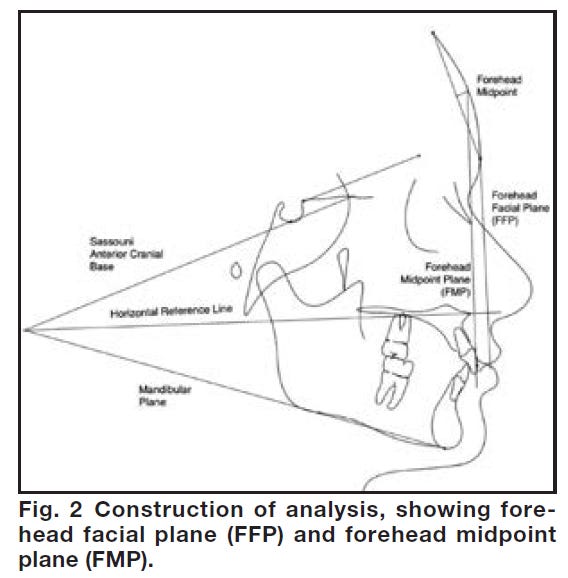
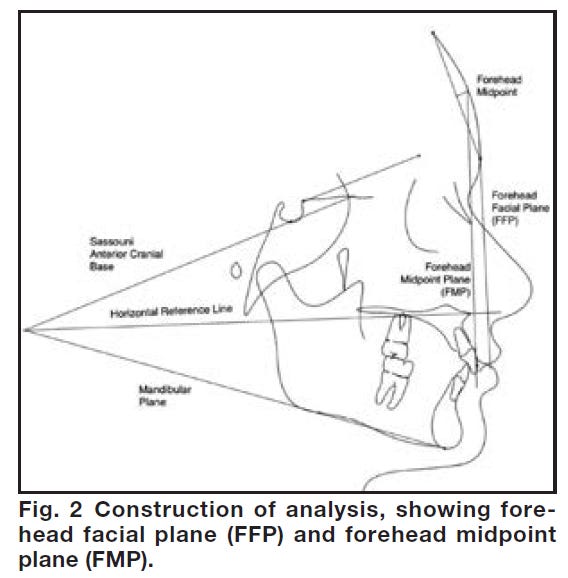
Forehead Facial Plane (FFP): Vertical line from glabella perpendicular to a horizontal reference plane.
Forehead Midpoint Plane (FMP): Vertical line from the midpoint of the trichion-glabella segment.
Measurements: Distances from the upper incisor to the FFP and FMP recorded to the nearest tenth of a millimeter.
Analysis
Statistical Tools: Matlab software for descriptive statistics and t-tests.
Measurement Reliability: Retesting of 10 subjects confirmed high consistency (Dahlberg error < 0.27mm).
Results
Key Measurements:
Females: Upper incisors positioned -2.2mm behind the FFP and 1.6mm anterior to the FMP.
Males: Upper incisors positioned -2.6mm behind the FFP and 3.4mm anterior to the FMP.
Combined Data: The ideal range for upper-incisor positioning lies behind the FFP and in front of the FMP.
Gender and Age Influence:
No significant differences were observed between genders (p > 0.05) or age groups (p = 0.087).
Variations in forehead morphology influence the acceptable range for incisor positioning.
Conclusion: The upper incisor's optimal position is bounded by the FFP and FMP for achieving an esthetically pleasing profile.
Clinical Cases
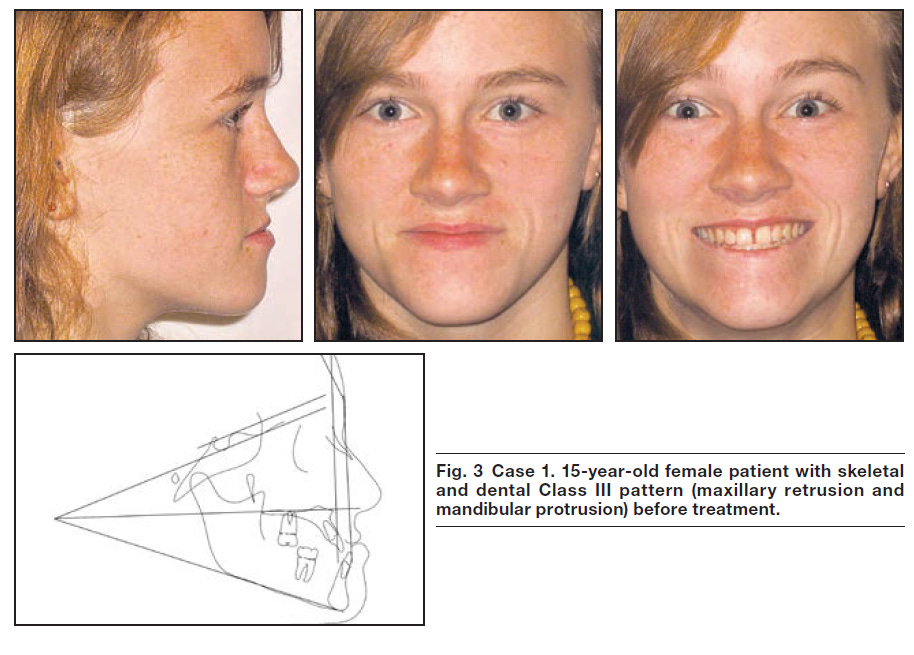
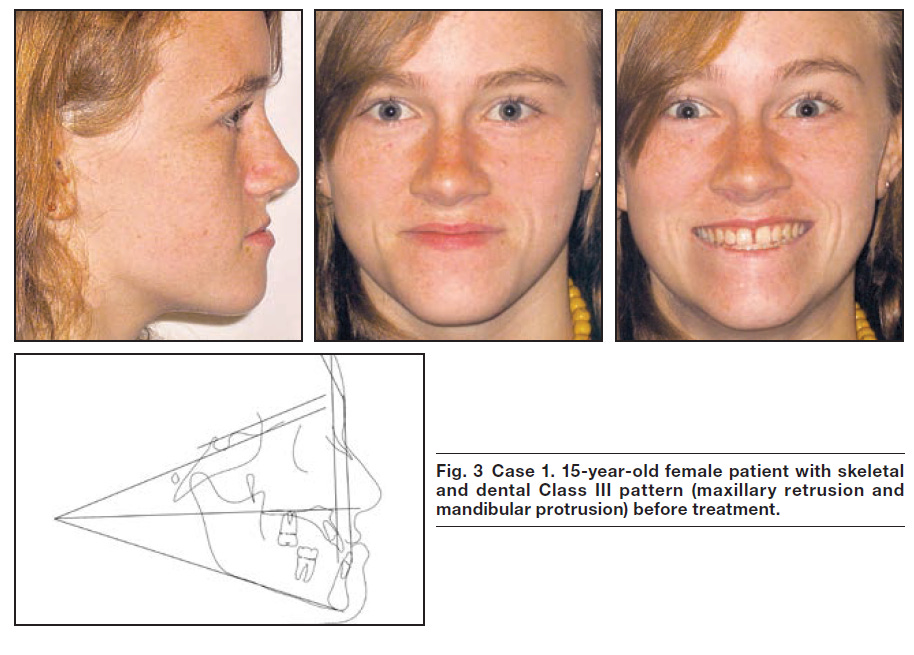
Case 1: Skeletal Class III with Mandibular Asymmetry
Patient: 15-year-old female.
Diagnosis: Maxillary retrusion, mandibular protrusion, mild asymmetry.
Treatment Plan:
Double-jaw surgery: 4mm maxillary advancement and mandibular retrusion/rotation.
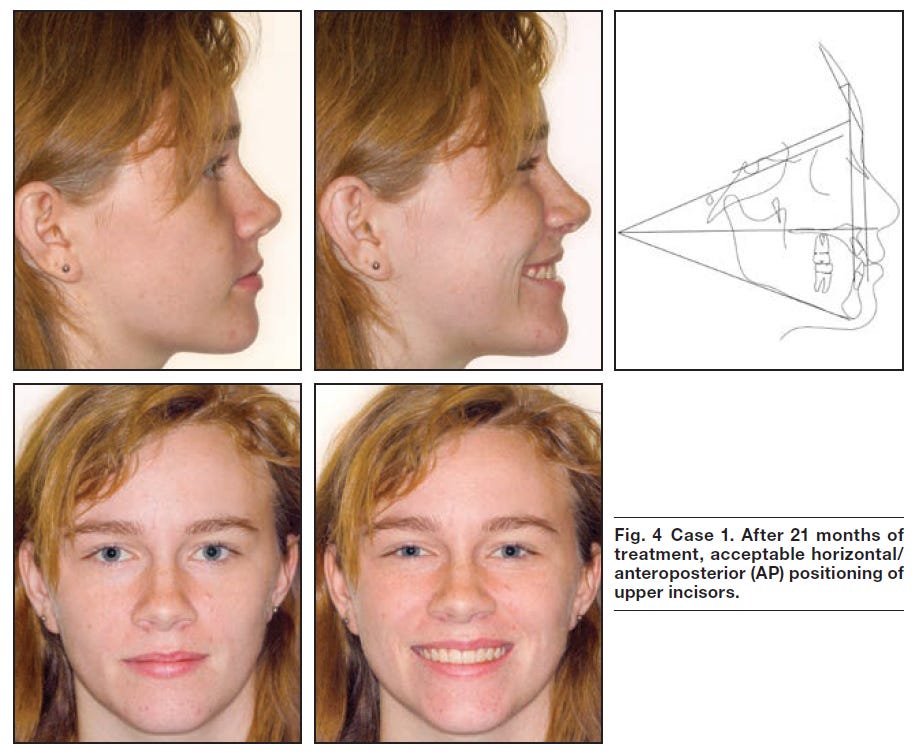
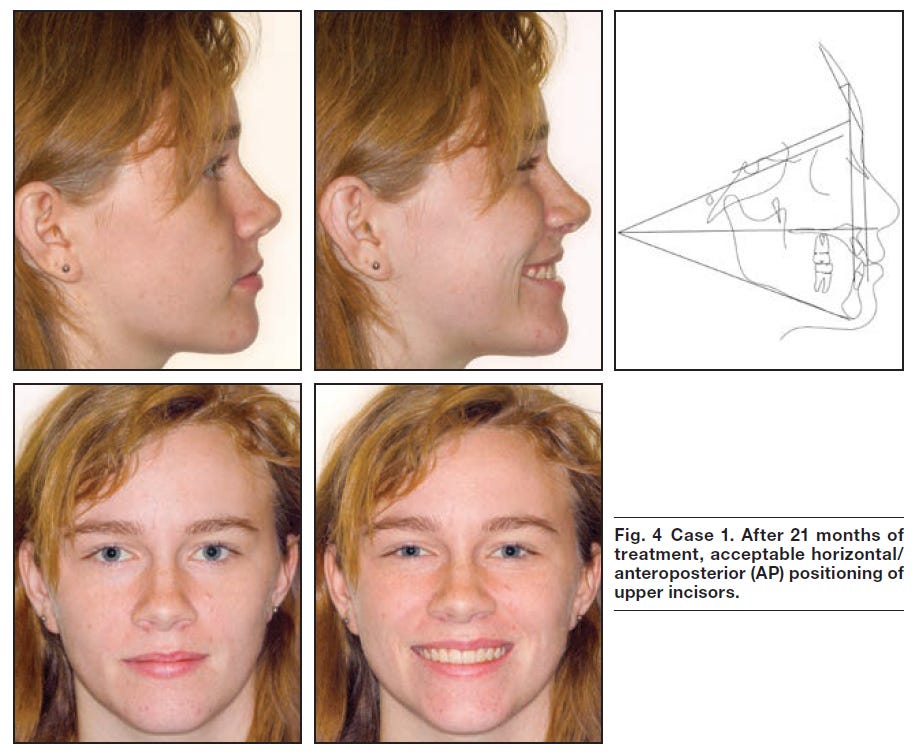
Orthodontic alignment over 21 months.
Outcome: Upper incisors aligned to the FFP, achieving balanced esthetics and functional occlusion.
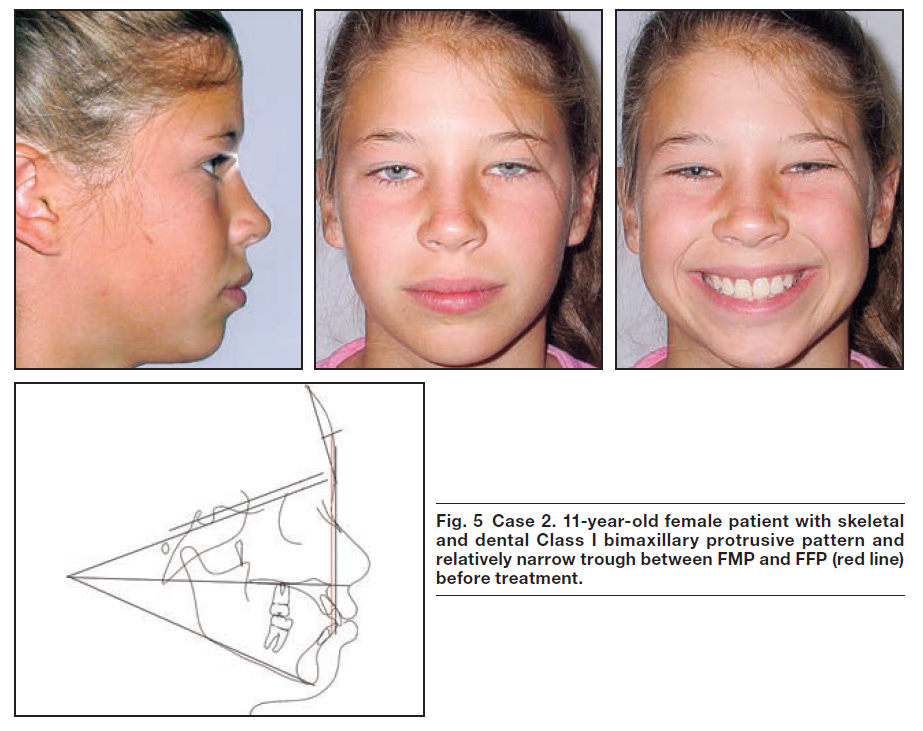
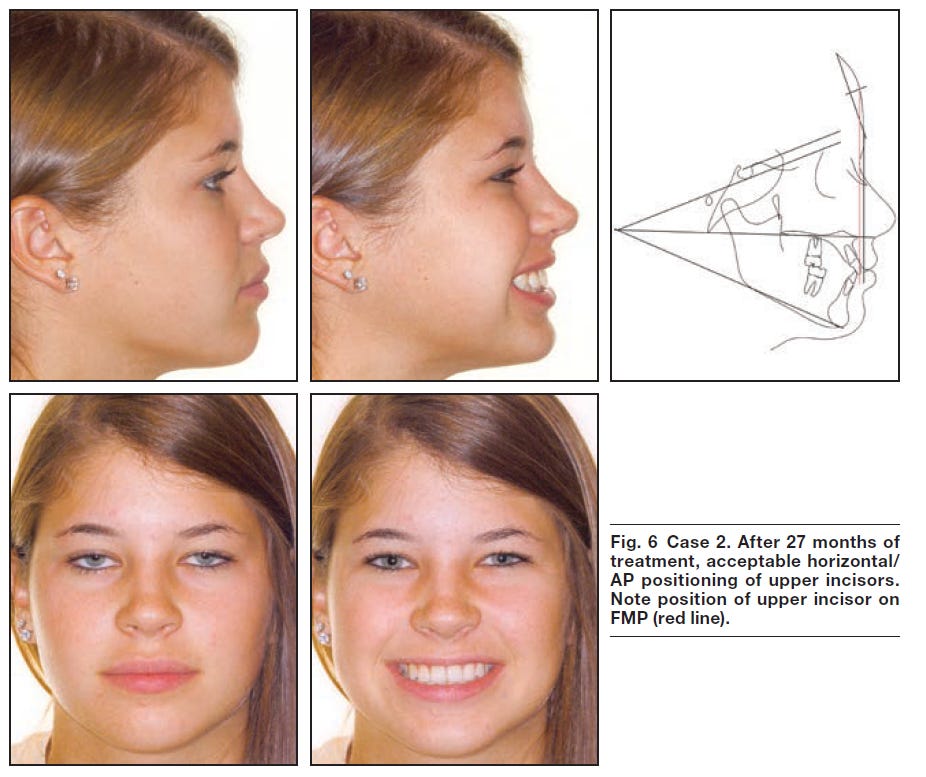
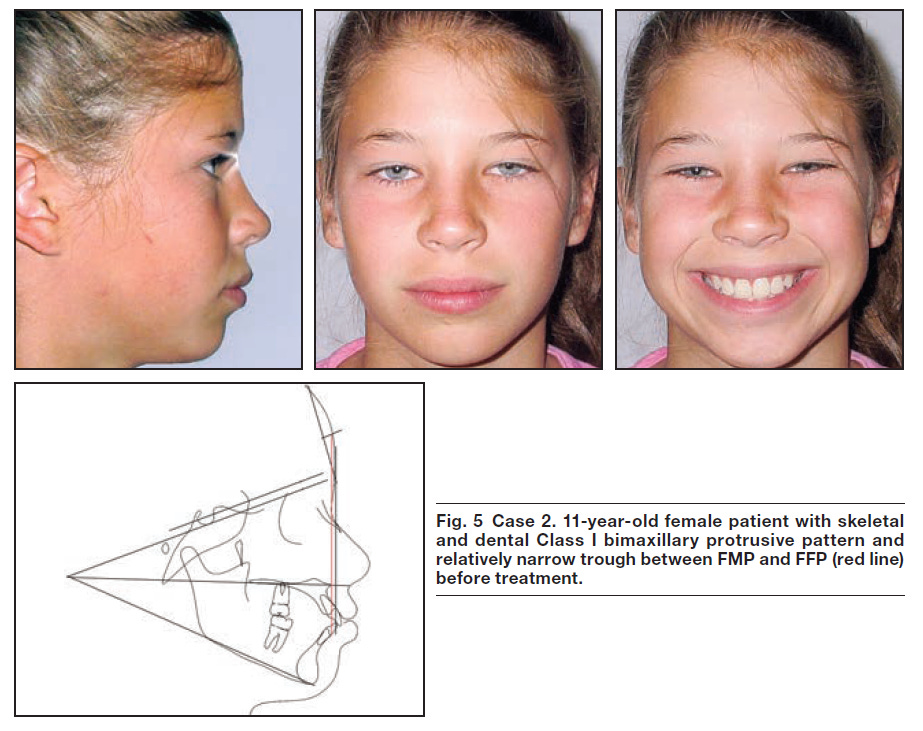
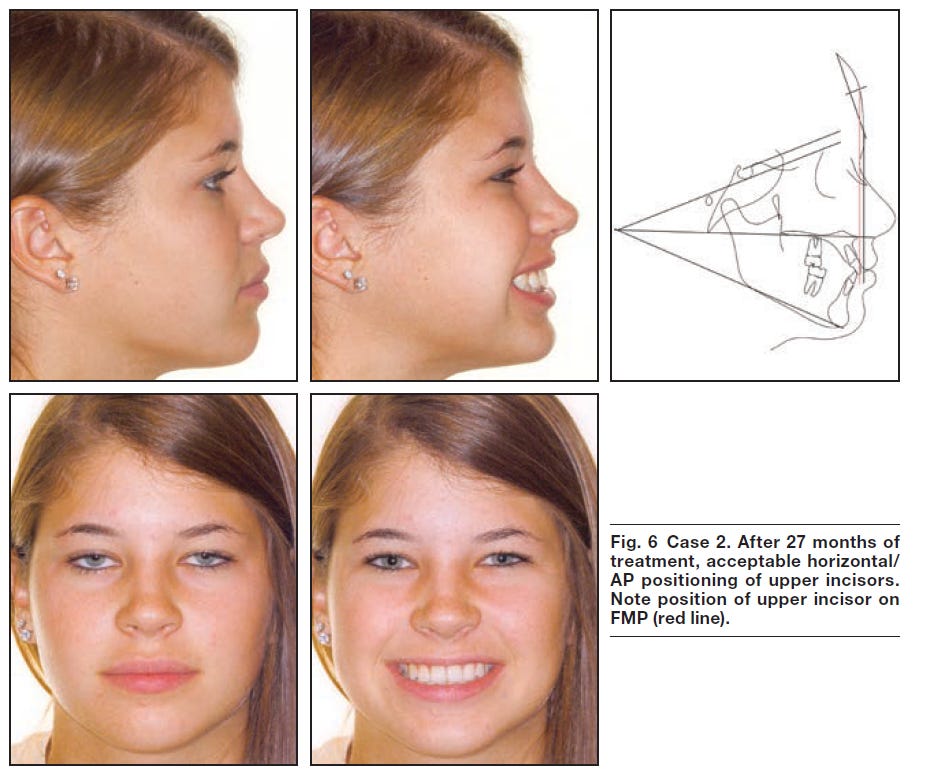
Case 2: Bimaxillary Protrusion
Patient: 11-year-old female.
Diagnosis: Skeletal and dental Class I with flared upper and lower incisors.
Treatment Plan:
Extraction of four first premolars for space creation.
Incisor retraction over 27 months.
Outcome: Upper incisors repositioned within the FMP and FFP bounds, significantly improving profile harmony
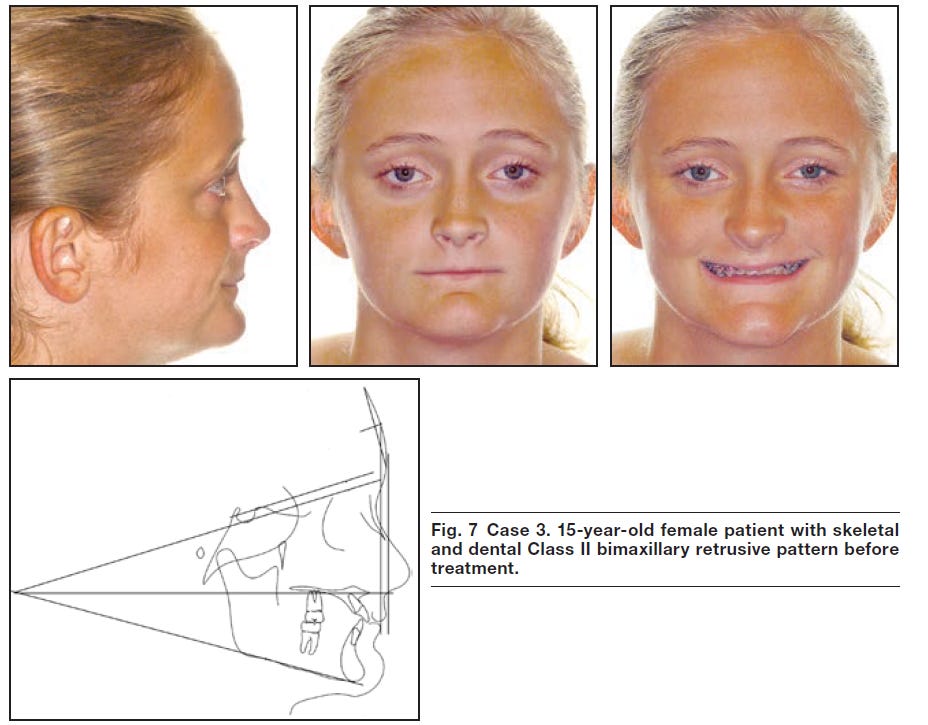
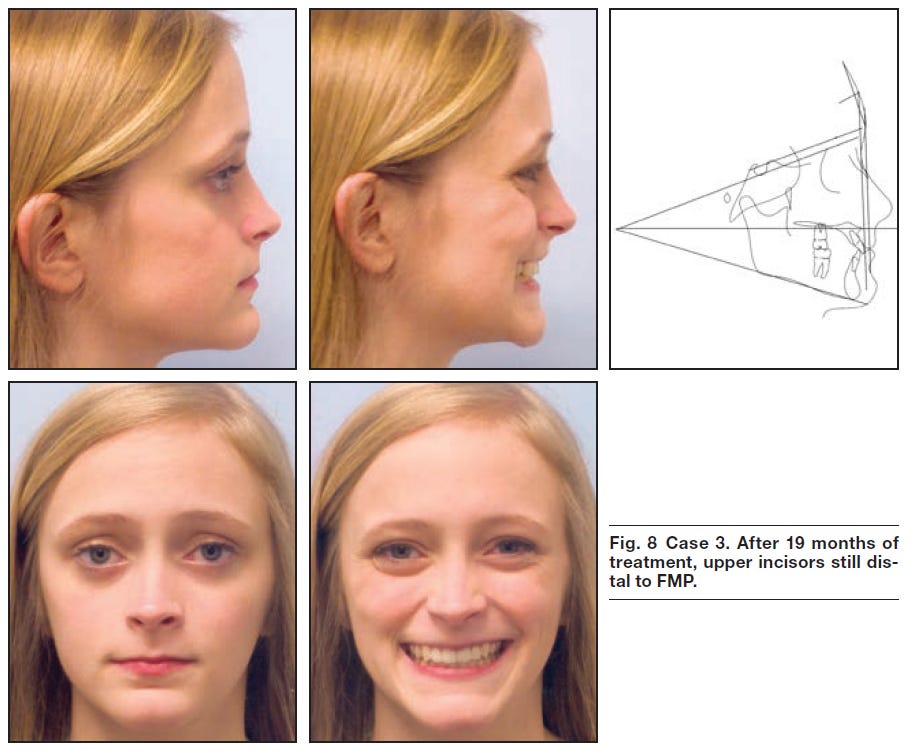
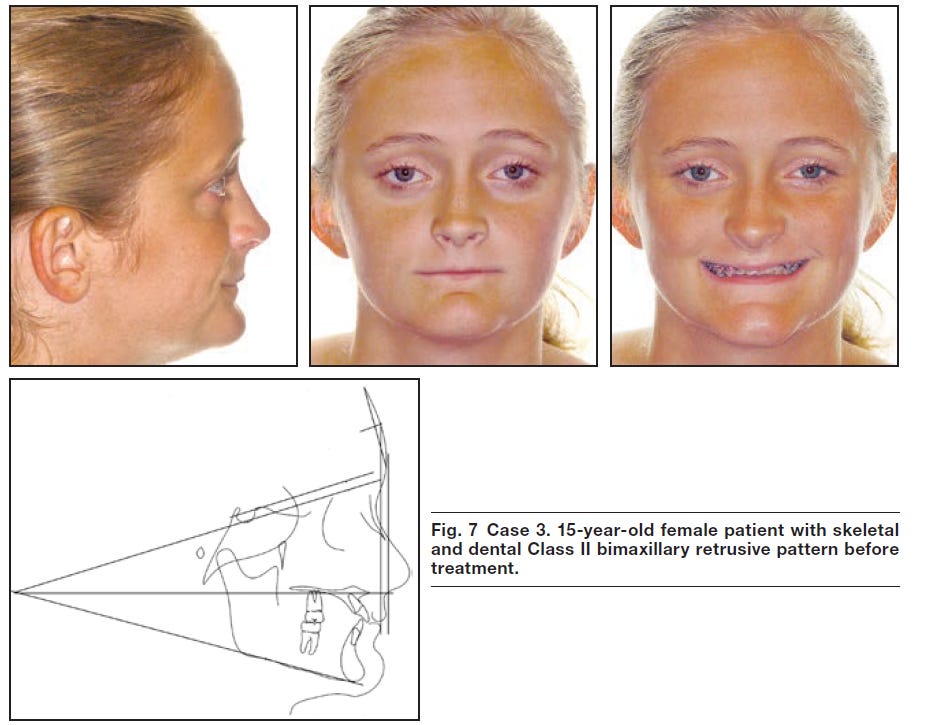
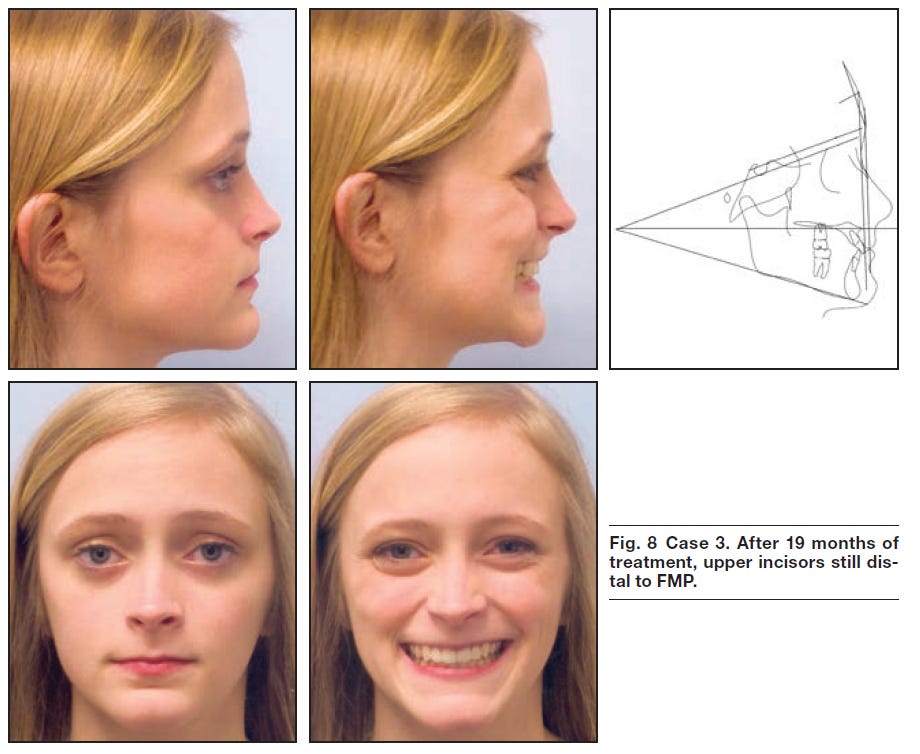
Case 3: Severe Skeletal Class II Bimaxillary Retrusion
Patient: 15-year-old female.
Diagnosis: Deficient AP position of maxilla and mandible, low facial height.
Treatment Plan:
Surgical advancement of both jaws with maxillary downgrafting.
19 months of orthodontic treatment.
Outcome: Despite improved AP relationships, additional maxillary advancement would have further enhanced lip support and profile esthetics.
Discussion
Comparison to Established Norms:
Ricketts E-Line: Lips typically positioned behind the E-line in pleasing profiles, consistent with Ricketts’ standards.
Holdaway Analysis: Confirmed the utility of integrating lip balance and incisor positioning for esthetic outcomes.
Role of Forehead Morphology:
More sloping foreheads allow forward incisor positioning.
"Feminine" profiles are sensitive to excessive incisor retraction, highlighting gender-specific considerations.
Broader Implications:
Accurate incisor placement supports vertical and AP profile balance, improving both esthetics and stability.
Incorporating soft-tissue landmarks offers an objective framework for both orthodontic and surgical treatment planning.
Conclusion
This study emphasizes the upper incisor's AP position as a critical determinant of facial harmony. Using soft-tissue planes such as the FFP and FMP allows for tailored treatment planning that accounts for individual variations in forehead morphology and gender differences. The findings reinforce the need for orthodontists to prioritize soft-tissue profiles in diagnostic and treatment strategies, ensuring superior esthetic and functional outcomes.