

Dental Impression Materials and Techniques
Amit Punj, BDS, DMD; Despoina Bompolaki, DDS, MS; and Jorge Garaicoa, DDS, MS

Introduction
This paper examines the key materials and processes used to capture precise negative impressions of teeth and oral tissues for the fabrication of indirect restorations. The authors stress that impression making requires both scientific knowledge and artistic skill. The correct understanding and handling of impression materials are crucial to achieving a well-fitting final prosthesis, whether fixed or removable.
Historical Perspective
From the 17th and 18th centuries—when wax, ivory, and bone impressions were used—to the introduction of modern polymers, impression materials have continuously evolved. Key milestones include:
Wax Impressions (17th–18th centuries)
Zinc Oxide Eugenol and Compound (limited by distortion)
Reversible Hydrocolloids (1925)
Irreversible Hydrocolloids (Alginates) (1941)
Elastomers like polysulfides, condensation silicones, and eventually polyether (late 1960s)
Polyvinyl Siloxane (PVS) (1970s), prized for its stability
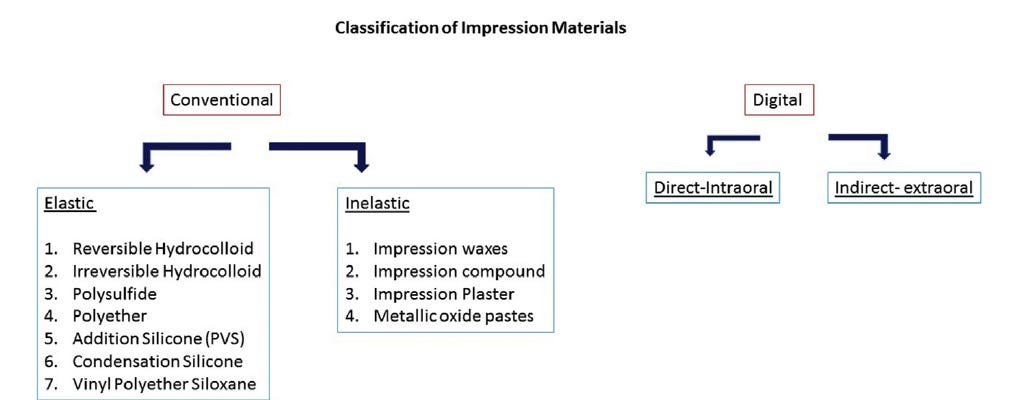
Classification of Impression Materials
Impression materials are frequently categorized by setting reaction and final properties. The elastomeric class includes:
Irreversible Hydrocolloids (Alginates)
Polyethers
Polyvinyl Siloxanes (PVS)
Alongside these, newer blends and variants address concerns of dimensional stability, moisture tolerance, and ease of mixing
Irreversible Hydrocolloids (Alginate)
Uses: Full-arch impressions for diagnostic casts, partial removable frameworks, interim dentures.
Advantages: Low cost, good wettability, and ease of mixing.
Limitations: Poor dimensional stability if not poured quickly (within 10 minutes), relatively low tear strength, and single-pour capability.
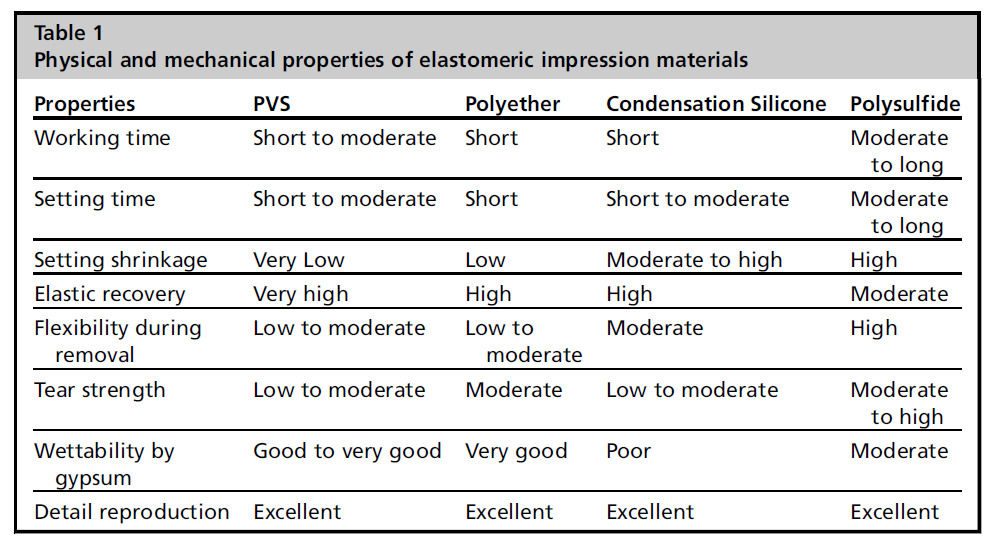
Polyethers
Setting Reaction: Cationic polymerization with no by-products.
Key Properties: Hydrophilic, excellent detail in a moist field, can be dispensed via motorized mixers.
Caution: Susceptible to distortion if submerged in water, especially longer than 30 minutes.
Polyvinyl Siloxanes (PVS)
Chemistry: Base paste (hydrosilane-terminated molecules) reacts with accelerator containing vinyl end groups.
Strengths: High dimensional stability, excellent elastic recovery, multiple pours possible.
Avoid Latex: Sulfur from gloves or retraction cords can inhibit polymerization.
Variants: Includes vinyl siloxanether (combining PVS and polyether properties), hydrophilic PVS, fast-set options, and alginate substitutes (medium-body PVS).
Disinfection of Conventional Impressions
Protocol: Rinse immediately, then spray or immerse in an appropriate disinfectant for a recommended time.
Effect on Material: Studies show minimal clinically significant changes if done correctly. Overly long immersion may degrade hydrocolloids or polyethers.
Wettability: Disinfectants can remove surfactants from PVS, increasing hydrophobicity unless mitigated by a wetting agent.
Gingival Displacement
Purpose: Provide an unobstructed view of the finish line and submarginal tooth structure. ~0.2 mm displacement is recommended for adequate impression material thickness.
Methods: Mechanical (cords), chemical (hemostatic agents), surgical (electrosurgery, laser), or combinations.
Cordless Techniques: Use an expanding synthetic polymer. Though less pressure is exerted on tissues, these can be less effective in deep subgingival cases. In general, both cord-based and cordless approaches can be equally effective with minimal periodontal trauma.
Tray Selection
Custom vs. Stock: Custom trays provide uniform material thickness, minimized distortion, and reduced material waste. Stock trays can be adequate for simpler or single-unit cases.
Dual-Arch Trays: The closed-mouth technique captures prepared tooth, opposing dentition, and occlusion in one step. Recommended for single units or short spans with stable occlusion. Rigid tray walls are crucial to prevent flexing.
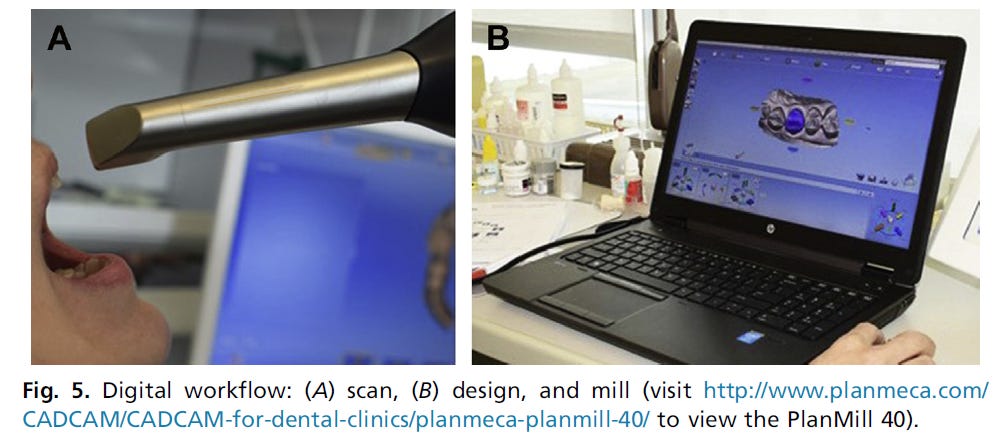
Digital Impressions
Digital technology is now mainstream, enabling:
Real-Time Visualization and the ability to correct scans immediately.
Paperless and Eco-Friendly approach, with no need for physical disinfection or storage.
Potential for Same-Day Restorations with in-office CAD/CAM milling or remote lab fabrication.
Hardware and Software Highlights
Common scanning systems (CEREC, PlanScan, 3M True Definition, Trios 3, iTero, CS3600) each have unique scanning principles, color/no-color capture, open/closed file formats, and user interfaces.
Clinical Indications: Excellent for single units and quadrant dentistry; full-arch accuracy remains a challenge.
Learning Curve: Some practitioners adapt quickly; others may find it steeper.
Future Outlook
The boundary between digital impressions, cone-beam CT, and advanced imaging (e.g., optical coherence tomography) is blurring. Systems are becoming faster, smaller, and more powerful. The authors anticipate a future where scanning directly penetrates soft tissues, capturing subgingival details without the need for a separate step. Sonography-based scanning could eventually bypass current limitations of optical impression systems, heralding a new era of streamlined dental workflows.
Summary/Analysis
Key Takeaways:
Material Selection: Polyethers, PVS, or alginate substitutes each address specific clinical demands (moisture, detail reproduction, cost).
Accurate Impressions: Achieved through proper disinfection, adequate gingival displacement, and correct tray or digital scanning technique.
Digital Leap: Intraoral scanning is increasingly favored for single or short-span restorations, though conventional methods remain widely employed and clinically valid.
Advancing Landscape: Rapidly evolving scanning and milling technologies promise more efficiency, accuracy, and better patient experiences.